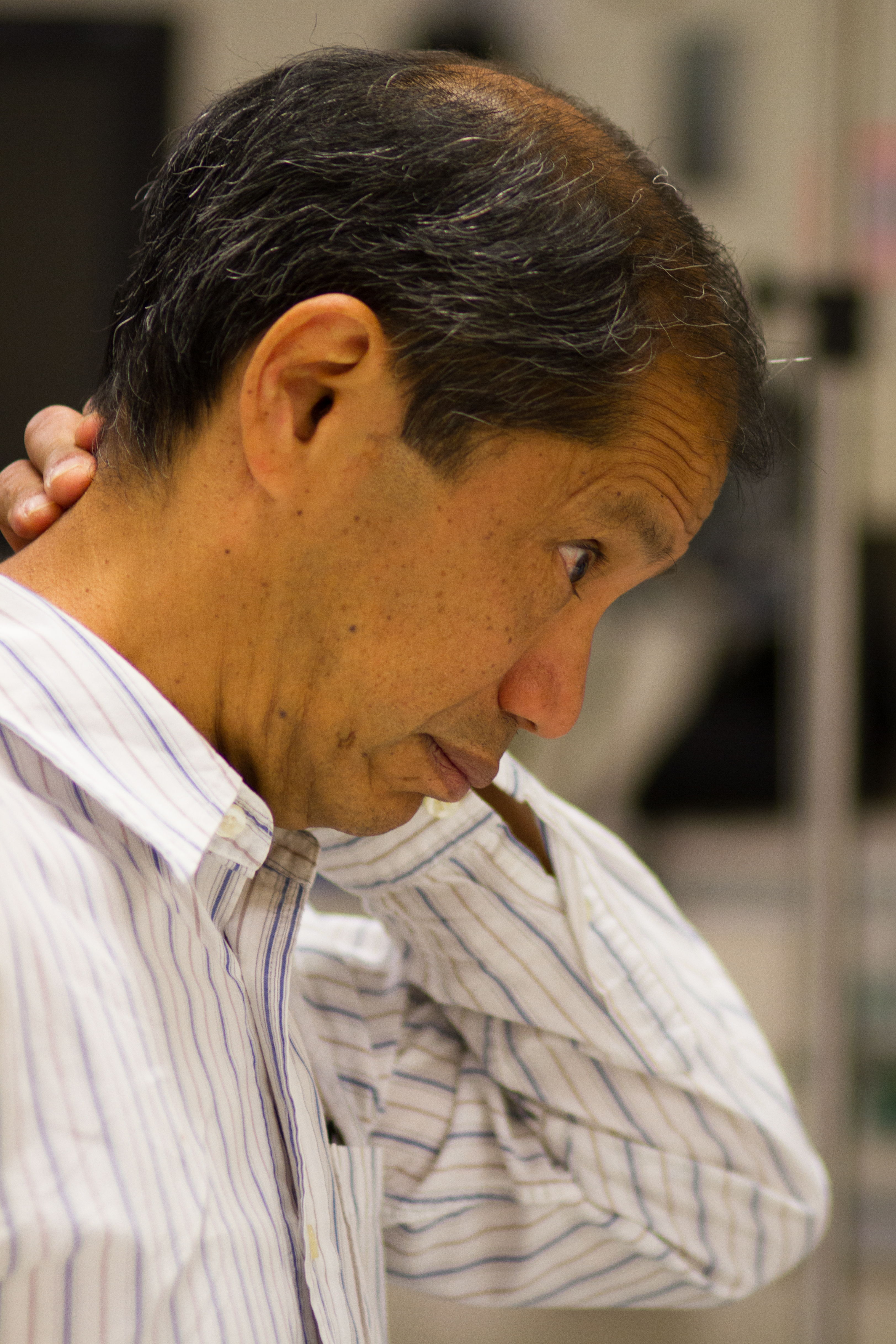
Margarita Castillo is a thin, frail 73-year-old Filipina female who presents with a history of multiple ground level falls in the previous week. This morning, her friend Mr. Flores, who lives down the street, became concerned when Mrs. Castillo’s newspaper was still on her front porch at 10 a.m. He went to check on her and found her on the floor and confused. He called 911 and she was taken to the emergency department (ED) in a cervical collar.

Please drag the bottom right corner to expand the box.

Photo courtesy of UW Medicine
1Advanced trauma life support (ATLS®): the ninth edition. ATLS Subcommittee et al. J Trauma AcuteCare Surg. (2013).
On arrival to the ED, Mrs. Castillo’s blood pressure (BP) is 92/48 mmHg, heart rate (HR) is 104 beats/minute (bpm), respiratory rate (R) is 8 breaths/min (bpm), and temperature (T) is 97.0°F. Pulse oximetry is 90% on supplemental oxygen at 2L/min via nasal cannula. She has shallow breaths with noted grimacing. An intravenous (IV) line was started by EMS and normal saline (NS) is currently running at 75 mL/hour. A Foley catheter is placed for accurate measurement of output.
On the neurological examination, her Glasgow Coma Score (GCS) is 15, and she is tangential in her speech, speaking in both English and Tagalog and is demonstrating word finding difficulty.

Listen to the conversation between Mr. Flores and the provider while she gathers information about Mrs. Castillo.



The Advanced Practice Provider’s (APP’s) or Physician’s priority is to complete the physical examination of the patient.
Please check your answers below:




Here is Mrs. Castillo’s problem list from when she first arrived in the ED:

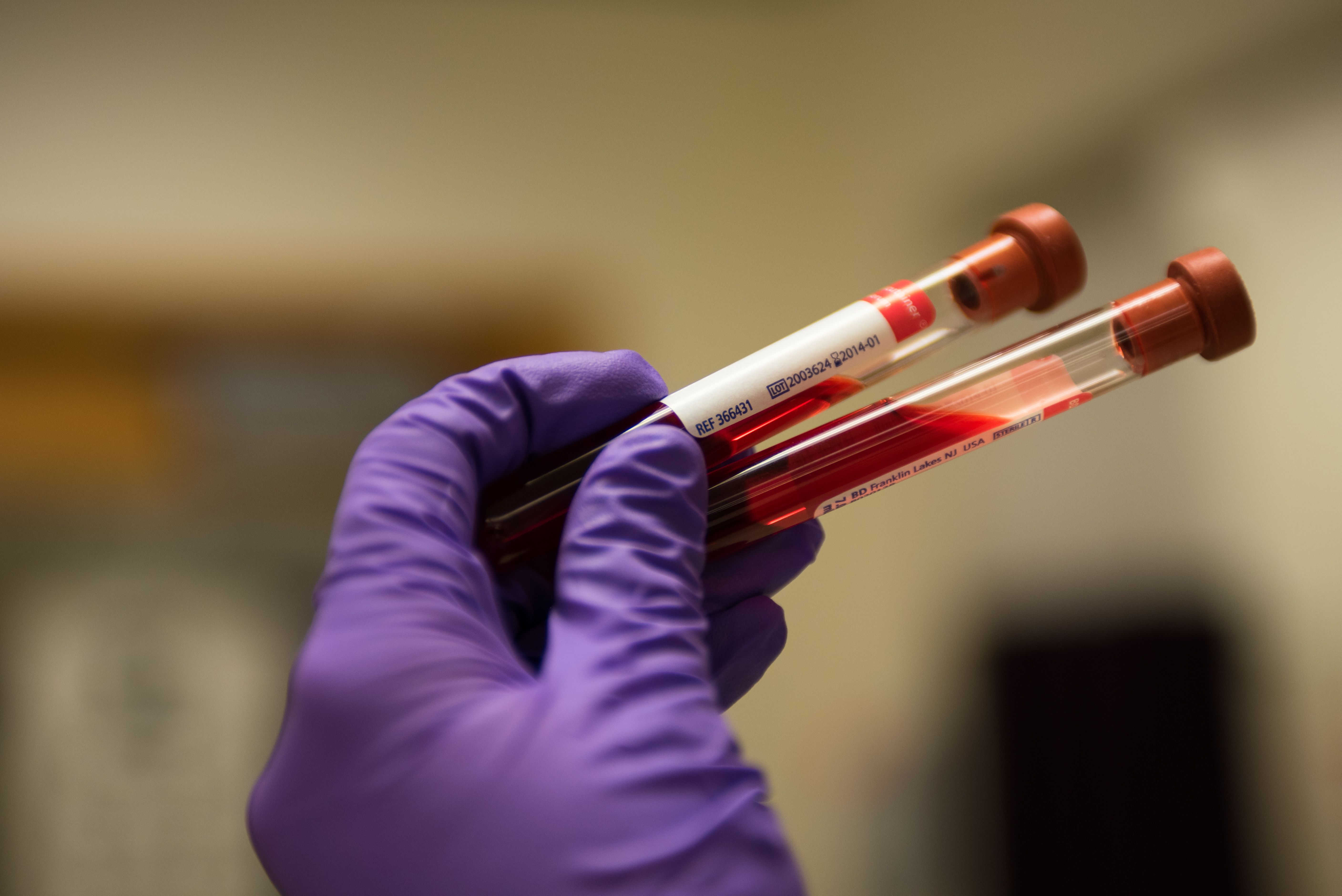
Photo courtesy of UW Medicine
The pharmacist’s priority is to review her medication and available medical history.


The social worker must balance respect for Mr. Flores and his desire to be included in the plan of care with Mrs. Castillo’s privacy. Mr. Flores, while a friend of Mrs. Castillo, is not legal next of kin. He must be treated considerately, but the social worker must also maintain Mrs. Castillo’s privacy and focus on locating legal next of kin.
Blood Alcohol Level: 0
INR: 1.0 (normal)
PTT: 35 seconds
CBC:
Hgb 9.9 g/dL
Hct 38%
Platelets 152,000/mm3
WBC 12,000 cells/mcL
Neutrophils 70% - Hi
Lymphocytes 23%
Monocytes 6%
Eosinophils 1%
Basophils 0.2%
BMP:
BUN 27 mg/dL
CO2 22 mmol/L
Creatinine 0.95 mg/dL
BUN/Creatinine Ratio: 28 - Hi
Glucose 310 mg/dL - Hi
Sodium 112 mEq/L - Lo
Chloride 85 mEq/L
Potassium 4.3 mmol/L
GFR calculated: 57.7 mL/min/1.73 m2 - Lo
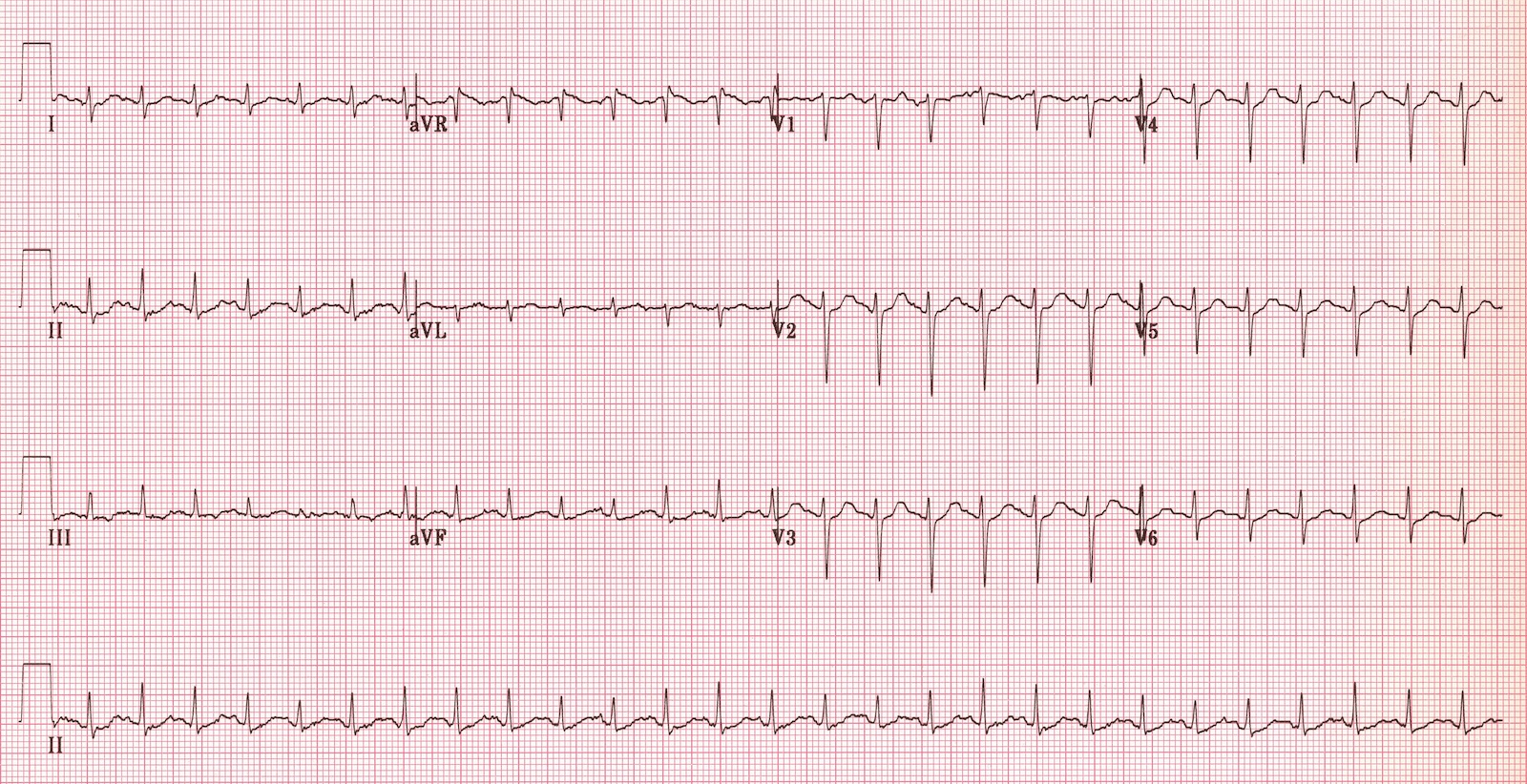
Troponin: 0.01 ng/mL negative
CK: 50 U/L
U/A- wnl, except for + protein
Urine Toxicology Screen-negative
Multiple left-sided rib fractures. Most of these appear to be chronic and healed; however, there are acute-subacute appearing fractures of the anterolateral aspect of the left 4th and 5th ribs. Ununited chronic fracture of the lateral aspect of the left 6th rib.
Spine CT: No fractures.
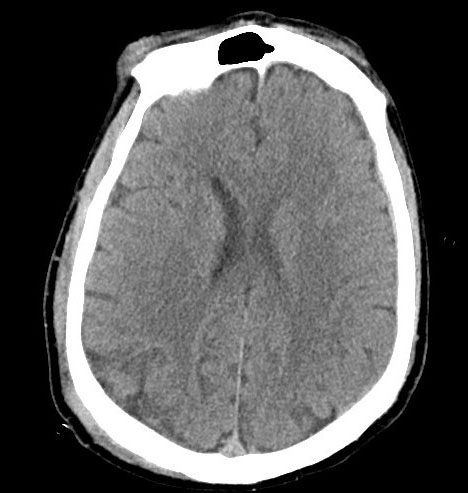
Head CT: 3mm right acute on chronic holohemispheric subdural hematoma without shift. No noted skull fractures.

Photo courtesy of UW Medicine.
The rationale for obtaining this consult is the presence of multiple rib fractures; need for assessment of possible elder abuse and locating legal next of kin (LNOK).
Social worker reports that she has attempted to contact patient’s daughter, but has not been able to reach her. Social worker will continue to reach out to daughter and locate other family members. Once family has been reached, social worker will conduct safety assessment for Mrs. Castillo, including assessing for possible elder abuse or neglect due to rib fractures.
The rationale for obtaining this consult is for surgical evaluation of the patient’s subdural hematoma.
Neurosurgery finds that the SDH is non-operable and recommends the transfusion of a 6-pack of platelets.
Aspirin therapy, such as Mrs. Castillo was receiving, disrupts platelet function by inhibiting COX-1 for the life of the platelet (~7-10 days). Presently, platelet transfusion for patients receiving antiplatelet agents, such as aspirin, is controversial and requires further study. A summary of work in this area is provided in the link below.