
In the third unit, Whole Person Narrative Patient-Centered Care, you will observe Wendy’s follow-up visit with her physician and her partner, Oscar, and explore the dimensions of whole person care, including spirituality.

". . . That business of the spirit, of the non-material self, of sympathy for and knowledge of others is the most important thing: in how we love, in how we live, and in what matters."
Colm Tóibín, writer and novelist
Each time chronically ill patients experience a serious medical incident they are confronted with their mortality and the associated issues of meaning and grief that are critical dimensions of the whole person experience.
Whole person care seeks to comprehend and address the physical, emotional, social, and spiritual dimensions of the person to relieve suffering and promote healing in acute and chronic illness.
Whole person care is focused on accepting a changed life and draws on the inner resources of the patient and family with the patient in control. Whole person care complements biomedicine which is controlled by the physician and focused on preserving life.
Hutchinson T 2011

... it sounds trite, yet I can only say that I realized for the first time that I don't have forever....
In the first stages of my illness, I couldn't sleep, urinate or defecate - the word ordeal comes to mind. Then when my doctor changed all this and everything worked again, what a voluptuous pleasure it was. With a cry of joy I realized how marvelous it is simply to function. My body, which in the last decade or two had become a familiar, no longer thrilling old flame, was reborn as a brand-new infatuation.
I realize of course that this elation I feel is just a phase, just a rush of consciousness, a splash of perspective, a hot flash of ontological alertness. But I'll take it, I'll use it. I'll use everything I can while I wait for the next phase. Illness is primarily a drama and it should be possible to enjoy it as well as to suffer it. I see now why the romantics were so fond of illness - the sick man sees everything as metaphor. In this phase I'm infatuated with my cancer. It stinks of revelation.
As I look ahead, I feel like a man who has awakened from a long afternoon nap to find the evening stretched out before me. I'm reminded of D'Annunzio, the Italian poet, who said to a duchess he had just met at a party in Paris, ''Come, we will have a profound evening.'' Why not? I see the balance of my life - everything comes in images now - as a beautiful paisley shawl thrown over a grand piano....
Read the full essay in the New York Times
Think of a loved one or patient with serious illness who you believe received good medical care even when medicine did not have a cure for their disease. What made their care “good”?
Click on the button up to see what most patients and families say.
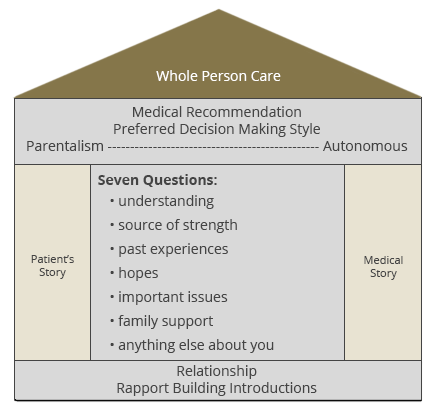
The Seven Questions presented in unit two will help you gain a deeper understanding of the whole patient and her family and ensures that the treatment you provide supports a meaningful life for everyone involved.

Lo, Ruston, Kates, et al. 2002
While Wendy’s nociceptive pain is controlled, she continues to describe a different kind of “pain” that doesn’t respond to her pain medications. It is a deep ache in her chest made worse when she thinks about what will happen to her grandchildren and her relationship with Oscar.
Treatment of nociceptive pain in cancer patients is a critical first step in addressing whole person pain. Continued support in dealing with the emotional, psychological and spiritual concerns of patients with advanced illness is also critical for treating the whole person’s pain.
At the end of the initial visit, the physician stated that he would like Oscar to participate in their next meeting to share his understanding of the situation so the three of them can work together.
Observe the differences in the attempts to set the context for the follow-up visit with Oscar and Wendy in the videos below. After watching each video you will be asked to identify the communication skills you observed.
Quite a lot happens during the three-way discussion with Wendy, Oscar and the primary care physician. Use the check list below to identify the communication skills that that were most effective in this interaction.
With experience, you will adapt the skills for Narrative Patient-Centered Care to your own personality and modify them as the situation requires.
As you will see, Wendy’s physician uses some, but not all, of the Seven Questions.
You will also notice that Oscar raises several important concerns before the physician asks about them. Some things he say surprise even Wendy.
Wendy’s physician does not shy away from discussing Oscar’s spiritual beliefs. He acknowledges Oscar’s beliefs without subscribing to them himself.
How do you feel about the physician’s approach?
Observe the differences in the attempts to summarize and confirm Oscar’s story in the videos below. After watching each video, you will be asked to rate the physician’s use of Narrative Patient-Centered communication skills.
Observe the differences in the attempts to create a shared narrative and a plan of care in the videos below. After watching each video, you will be asked to rate the physician’s use of Narrative Patient Centered communication skills.
In the third unit, Whole Person Narrative Patient-Centered Care, you observed Wendy’s follow-up visit with Oscar and her primary care physician. You saw that managing Wendy’s whole person care included both nociceptive pain control and attention to the other important issues that were causing her distress.
The communication skills learned in the third unit were used to deepen and extend the narrative approach during the follow-up visit, including spiritual issues.

Hutchinson T. “Whole person care. In: Whole Person Care: A New Paradigm for the 21st Century. Hutchinson T, Ed. New York: Springer 2011.
Lo, Ruston, Kates, et al. Discussing Religious and Spiritual Issues at the End of life: A Practical Guide for Physicians. JAMA Feb 13, 2002-Vol 287, No. 6: 749754.
© 2015 University of Washington | School of Nursing | L&IT Learning Technologies | Palliative Care Training Center
